

What is Myofascial Release?
Myofascial Trigger Points (TrPs)—commonly known as “muscle knots”—are one of the most frequent yet misunderstood causes of chronic pain. Because they often manifest as referred pain (pain felt in a different location from the actual source), they are frequently misdiagnosed as nerve issues, sinus infections, or structural damage.
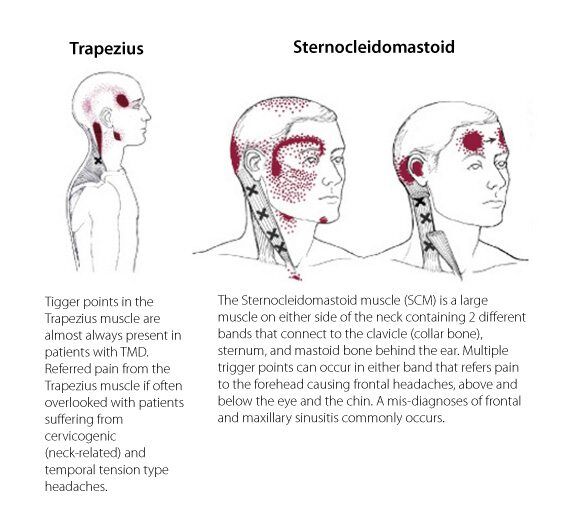
Consider the case of Jane, who suffered for years from debilitating headaches, molar pain, and dizziness. Despite multiple scans and nerve tests, the cause remained a mystery until a physical examination revealed trigger points in her Sternocleidomastoid (SCM) muscle—a thick muscle in the front of the neck.
While Jane’s neck never felt “sore,” the knots in her SCM were sending pain signals upward to her eye, cheek, and ear. This is the hallmark of myofascial pain: the source is often silent, but the “echo” is loud and distracting.
Symptoms Of Myofascial Trigger Points
The most fascinating aspect of trigger points is their predictable referral patterns. Pioneers Dr. Janet Travell and Dr. David Simons mapped these patterns, proving that trigger point pain does not follow “dermatomes” (the pathways of single spinal nerves).
While radiculopathy (a pinched nerve) follows a specific nerve root path, trigger point pain is ubiquitous and can mimic other conditions. This is why a patient might visit a dentist for a toothache, only to find the “culprit” is actually a trigger point in their masseter (jaw) muscle, or seek treatment for an earache that is actually originating from the neck.
The “Masqueraders” of Pain
Trigger points are often the “great masqueraders” in clinical practice. Because they refer pain to distant sites, they are frequently misdiagnosed as other syndromes:
Pseudo-Carpal Tunnel: A trigger point in the subscapularis (a muscle in your armpit) can refer pain all the way down to the wrist, perfectly mimicking Carpal Tunnel Syndrome even when the median nerve is perfectly healthy.
Referred Back Pain: While we often look at the spine for lower back pain, the source could surprisingly be trigger points located in the abdominal muscles (stomach), the glutes (buttocks), or even the calf muscles.
Autonomic Symptoms: Beyond just pain, these “knots” can trigger autonomic responses. It is not uncommon for a trigger point to cause localized sweating (perspiration), watery eyes (nasal secretions), nausea, or even dizziness.
So What Are Myofascial Trigger Points?
To truly understand why a “knot” in your neck can cause a “pain” in your forehead, we have to look at the unique mechanics of myofascial trigger points. Unlike general muscle tightness, a trigger point is a localized physiological “traffic jam” that creates a self-sustaining cycle of pain known as a Metabolic Crisis.
The Anatomy of a “Metabolic Crisis”
This crisis begins when a small patch of muscle fibers stays contracted, acting like a vice that chokes off the microscopic blood vessels, or capillaries, in that specific spot. This restriction of blood flow—medically known as ischemia—prevents the “trash” produced by the muscle (metabolic waste) from being hauled away.
As these toxins accumulate, they create a highly acidic environment that irritates local nerve endings. These irritated nerves send a signal to the brain that the tissue is in trouble; however, the brain responds by telling the muscle to contract even harder to “protect” the area. This reflex creates a vicious cycle: the increased contraction further restricts blood flow, which leads to more toxins, more irritation, and an even tighter knot.
Identifying the “Taut Band”
Clinically, a physiotherapist identifies a trigger point through precise manual palpation. It is distinct from general muscle tension because it resides within a taut band of tissue—often described by patients as feeling like a “guitar string” buried under the skin. Within this band, the therapist can feel a hard, pea-sized nodule which is the actual trigger point.
When a therapist applies pressure to this nodule, it often elicits a local twitch response, where the muscle visibly jumps. More importantly, this pressure reproduces the patient’s familiar referred pain, sending a sensation to a distant site that confirms the true source of the discomfort.
Treating Myofascial Trigger Points
Effective treatment for myofascial trigger points goes beyond surface-level massage, utilizing a multi-layered clinical approach to achieve lasting relief. While various techniques exist, manual compression is highly effective because it allows a therapist to precisely isolate a hardened nodule and its associated taut band. By applying sustained pressure, the therapist essentially “resets” the muscle’s neural signaling through gamma motor control. This neurological intervention prompts an overactive, shortened muscle to finally relax, while simultaneously improving the recruitment of surrounding muscles that may have become weak or inhibited.
However, the key to permanent recovery lies in identifying and correcting the original “drivers” of the trigger point. While deactivating a knot provides immediate comfort, the muscle will inevitably return to its strained state if underlying issues—such as poor ergonomic habits, structural variations, or muscle imbalances—remain unaddressed. True resolution requires combining direct tissue release with a strategy to fix the mechanical stresses that forced the muscle into a metabolic crisis in the first place.
The Role of Myofascial Release
Understanding Myofascial Release requires looking at the critical relationship between the muscle (“myo”) and the fascia—the fluid, three-dimensional connective web that supports your entire musculoskeletal structure. In a healthy state, this tissue is supple and glides effortlessly, but physical trauma, inflammation, or habitual poor posture causes the fascia to thicken and tighten. Over time, these restrictions act like a “straightjacket” around your muscles, choking off blood flow and trapping the body in a cycle of chronic stiffness.
Because the fascial network is entirely interconnected, a restriction in a single area, such as the mid-back, can pull on the rest of the web, triggering seemingly unrelated symptoms like tension headaches or neck pain.
Myofascial Release is a specialized therapy designed to “melt” these specific restrictions. By using slow, sustained, and deep pressure, this technique allows the fascia to elongate and return to its natural, elastic state. By addressing the tissue at this foundational level, we can effectively treat the root causes of stubborn conditions, including:
- Chronic Low Back Pain
- Persistent Headaches
- Sports Injuries
- General Neck Stiffness
At Core Concepts Singapore, we don’t just treat the pain you feel; we address the fascial restrictions that keep it there. If you’re struggling with stiffness that won’t go away, our specialist physiotherapists can help unbind your movement and restore your body’s natural flow.
References:
- The Trigger Point Therapy Workbook, by Clair Davies and Amber Davies
- Myofascial Pain and Dysfunction: The Trigger Point Manual by David Simons, Janet Travell, Lois Simons
- Archives of Physical Medicine and Rehabilitation, 2008
- New Views of Myofascial Trigger Points: Etiology and Diagnosis, Archives of Physical Medicine and Rehabilitation 2008
